How heat, labour, and pregnancy are quietly underwriting India’s climate response
Over the past decade, India has invested substantial political and administrative capital in constructing a national and sub-national architecture for climate governance, anchored in the National Action Plan on Climate Change (NAPCC), reinforced through the National Disaster Management Authority’s (NDMA) preparedness frameworks, operationalised through state-level Heat Action Plans, and more recently extended into the public health domain through the National Action Plan on Climate Change and Human Health. These initiatives reflect a genuine institutional recognition that climate change is no longer a distant environmental concern but a systemic risk to health, livelihoods, and development outcomes, and there is credible evidence that some of these interventions, particularly early warning systems for extreme heat and improved disaster response mechanisms, have saved lives.
At the same time, the dominant framing of climate risk within policy continues to privilege acute events, visible system stress, and measurable losses, with success often defined in terms of avoided mortality, protected infrastructure, and the speed with which services are restored after disruption. This framing, while necessary, remains incomplete. It systematically underrepresents forms of harm that accumulate gradually, operate below crisis thresholds, and are absorbed at the household or individual level rather than by institutions. Nowhere is this gap more consequential than in how women’s health, and particularly women’s reproductive health, is positioned within India’s climate response.

For millions of women across rural and peri-urban India, climate change does not primarily manifest as an episodic disaster that overwhelms systems and triggers emergency relief; it manifests as a steady modifier of everyday life, reshaping patterns of labour, access to basic services, healthcare utilisation, and reproductive decision-making under conditions of economic uncertainty. These shifts rarely appear as policy failures because they do not result in system collapse. Instead, they are internalised, managed privately, and rendered statistically invisible.
This essay argues that India’s climate and health policy frameworks, while increasingly sophisticated and well-intentioned, continue to rely implicitly on this internalisation, with women’s bodies, and particularly women’s reproductive health, functioning as unacknowledged buffers that absorb climate-related stress, which current indicators and programme designs are not calibrated to detect.
Gendered Labour, Heat Exposure, and the Reconfiguration of Reproductive Risk
Women’s exposure to climate stress in India is shaped less by geography alone and more by the social organisation of labour, particularly in rural and low-income contexts where women continue to perform the majority of unpaid domestic and care work alongside significant participation in agriculture and informal employment. These responsibilities place women in sustained contact with environmental stressors such as heat, water scarcity, and physical exertion, often without access to protective infrastructure, regulatory safeguards, or meaningful choice about withdrawal from work.
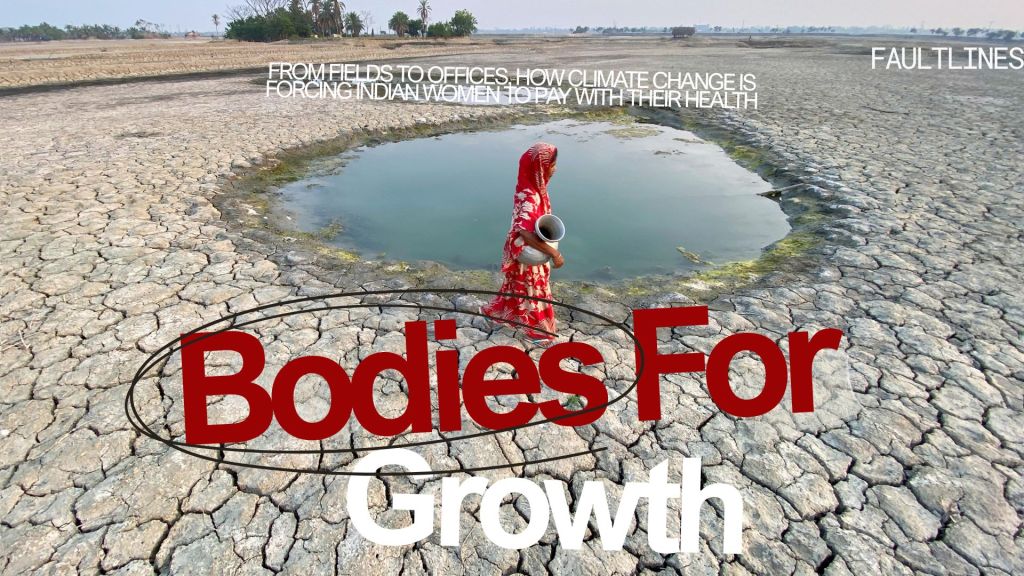
Empirical evidence illustrates the scale of this exposure. Data from the India Human Development Survey, 2011-12, shows that women spend nearly twice as much time as men collecting water, a burden that has intensified as groundwater depletion and rainfall variability increase across large parts of the country. States such as Rajasthan, Maharashtra, Bihar, Odisha, and Telangana, which already face chronic water stress, have experienced further pressure as climate variability deepens, forcing women to travel longer distances and make more frequent trips simply to meet basic household needs.

At the same time, the India Meteorological Department data indicate a marked rise in the frequency, duration, and geographic spread of heatwaves over the past two decades, with recent summers recording sustained temperatures above 45 degrees Celsius across large parts of north and central India, conditions that are physiologically punishing for anyone engaged in outdoor or physically demanding labour.
The health implications of this convergence are rarely captured in policy design. NFHS-5 shows that over 57 % of Indian women aged 15–49 are anaemic, with prevalence among pregnant women exceeding this national average in several states, a baseline condition that significantly reduces tolerance to heat stress, dehydration, and prolonged physical exertion. ORF’s analysis of gendered climate vulnerability emphasises that climate change does not create entirely new health risks in isolation but systematically amplifies existing nutritional and physiological vulnerabilities by increasing exposure intensity and workload.
CSIS’s work on climate and health in India reinforces this point by showing that climate vulnerability is socially produced, following patterns of labour and responsibility rather than hazard maps alone, meaning that women absorb climate exposure not simply because of where they live but because of the work they do to sustain households and informal economies.
It is within this context of accumulated strain that pregnancy unfolds, not as a protected physiological state but as another demand layered onto labour that cannot pause. India records approximately 25 million births each year, most of them among women whose lives are structured around informal employment, limited income security, and constrained access to healthcare. While NFHS-5 reports that institutional deliveries now exceed 88 %, this aggregate success masks a more fragile reality, because only 58.6 % of women receive four or more antenatal visits, and coverage is significantly lower in districts characterised by higher climate variability, poorer transport connectivity, and greater dependence on climate-sensitive livelihoods.
Pregnancy under these conditions becomes something that must be negotiated rather than safeguarded. Extreme heat increases the physical cost of travel to health facilities, floods disrupt transport and outreach, and income volatility raises the opportunity cost of seeking care, leading women to delay antenatal visits not out of ignorance but out of necessity. These delays feel rational at the household level, yet pregnancy is acutely sensitive to timing, and antenatal care cannot be compressed or recovered later without consequence. Missed windows for supplementation, screening, and referral do not announce themselves as failures in the moment, which is precisely why they are allowed to accumulate without triggering policy response.
Nutrition follows a similar logic of adjustment. Climate-induced price volatility and livelihood stress alter intra-household food allocation, and women routinely reduce their own intake first, prioritising children and working household members, a pattern consistently documented in NFHS and nutrition surveys. During pregnancy, when nutritional requirements increase, these compromises compound existing anaemia and increase the likelihood of low birth weight and other adverse outcomes. These effects manifest clinically but are rarely attributed to climate-related disruptions.
Policy Architecture, Programme Design, and the Persistence of Blind Spots
It would be inaccurate to characterise India’s response to climate risk as one of neglect. The National Action Plan on Climate Change laid the foundation for integrating climate considerations into development planning, while the National Disaster Management Authority’s evolving guidelines have strengthened preparedness and response to extreme events. State-level Heat Action Plans, particularly in cities such as Ahmedabad, have demonstrated measurable reductions in heat-related mortality through early warning systems, public communication, and interdepartmental coordination. The National Action Plan on Climate Change and Human Health represents an important step toward explicitly linking climate change with public health outcomes.
Yet these frameworks are largely calibrated to detect and respond to acute stress, visible system overload, and immediate mortality risk. Reproductive health impacts, by contrast, are characterised by gradual deterioration, disrupted continuity of care, and probabilistic increases in risk rather than sudden failure. As a result, they remain weakly integrated into climate response protocols.

Evidence synthesised by CSIS shows that utilisation of maternal health services declines immediately following climate shocks, even when health facilities remain operational, driven not by infrastructure damage but by transport disruption, income stress, and behavioural adaptation. Because utilisation typically rebounds in subsequent months, these disruptions disappear into annual averages, reinforcing a narrative of system resilience while masking the private costs borne by women during pregnancy.
India’s flagship health and nutrition programmes illustrate this misalignment. The National Health Mission has significantly expanded maternal health coverage, yet its monitoring frameworks prioritise contact and completion rather than continuity and timing, limiting their ability to detect climate-related disruption.
PM-JAY and state insurance schemes such as Aarogyasri, Telangana, provide financial protection against catastrophic health expenditure but offer little safeguard against the access disruptions that define climate vulnerability for pregnant and migrant women. ICDS and POSHAN Abhiyaan address maternal and child nutrition at scale, but their effectiveness depends on regular access to anganwadi services, which are frequently disrupted during floods, heatwaves, and seasonal migration.
Digital health initiatives, including the Ayushman Bharat Digital Mission (ABDM), hold promise for improving continuity of care, yet climate risk and mobility are not explicit design parameters, constraining their capacity to address climate-driven fragmentation of care pathways. In effect, current programme architectures assume stability at precisely the moment when instability is becoming the norm.
What emerges is not an absence of policy, but a misalignment between the forms of harm climate change produces and the forms of harm policy is designed to see.

Where Climate Stress Looks Different But Cuts Just As Deep: Urban Women, Heat, Housing, and Care
The assumption that climate vulnerability is primarily rural has also obscured how urban women experience climate stress in distinct but equally damaging ways, particularly in India’s rapidly expanding cities, where heat exposure, inadequate housing, informal employment, and fragile access to services converge to produce forms of risk that are less visible but no less consequential.
India’s cities are warming faster than surrounding rural areas due to the urban heat island effect, and data from the India Meteorological Department (IMD) shows that cities such as Delhi, Ahmedabad, Nagpur, Hyderabad, and Chennai now experience prolonged periods of extreme heat that are both more intense and more persistent than in previous decades, conditions that disproportionately affect women living in informal settlements with poor ventilation, limited access to water, and unreliable electricity.
According to Census and NSS data, a large proportion of urban women are employed in informal and semi-informal occupations, including domestic work, home-based manufacturing, street vending, sanitation, and care work, roles that require long hours, physical effort, and continuous mobility across the city, often during peak heat.
For these women, climate stress is not limited to exposure at work but extends into the home, where overcrowded housing, tin or asbestos roofs, and inadequate cooling make rest and recovery during pregnancy or illness difficult, if not impossible. Studies cited by CSIS note that urban heat exposure is increasingly associated with adverse health outcomes not because of outdoor labour alone, but because night-time temperatures remain elevated in dense settlements, disrupting sleep, hydration, and physiological recovery, particularly for pregnant women.
Urban pregnancy unfolds under a different but equally constraining set of pressures. While cities offer greater proximity to health facilities, access remains uneven, with migrant and low-income women facing barriers related to documentation, cost, and time. NFHS-5 data shows that urban averages mask sharp intra-city inequalities in antenatal care utilisation, with women in informal settlements significantly less likely to complete recommended antenatal visits despite geographic proximity to services.
Heatwaves exacerbate these barriers by increasing the physical cost of travel, overcrowding public transport, and reducing the flexibility of women employed in informal jobs where absence can result in immediate income loss or job termination.
Nutrition insecurity in cities further complicates this picture. Unlike rural households that may rely partially on subsistence production, urban poor households are entirely market-dependent for food, making them acutely sensitive to climate-induced price volatility. POSHAN Abhiyaan and ICDS services, while present in urban areas, often struggle to reach migrant populations consistently, and disruptions caused by heatwaves, floods, or evictions can interrupt access to supplementary nutrition at precisely the moments when pregnant women need it most.

Government responses have begun to acknowledge urban vulnerability through city-level Heat Action Plans and urban health missions, and there is evidence that early warning systems and public advisories have reduced heat-related mortality in some cities. However, these interventions remain largely focused on emergency response and public awareness rather than on integrating heat and climate risk into routine maternal and reproductive health planning. Urban health programmes, including the National Urban Health Mission, rarely treat extreme heat, housing conditions, or informal employment as determinants of reproductive health risk, reinforcing a separation between climate policy and women’s everyday health realities.
The result is that urban women, like their rural counterparts, absorb climate stress through delayed care, compromised nutrition, continued labour during pregnancy, and limited capacity for rest, but they do so in environments where vulnerability is masked by proximity to services and higher aggregate indicators, allowing climate-related harm to remain statistically invisible even as it accumulates inside bodies.
Climate Stress Behind Glass Walls: Corporate Women, Heat, Work Culture, and Invisible Risk
Climate vulnerability among Indian women does not disappear with formal employment, higher income, or access to air-conditioned offices; it is reorganised, masked by comfort, and reframed as individual coping rather than structural exposure, particularly among corporate and professional women whose work environments appear insulated from environmental stress but whose bodies remain deeply entangled with it. India’s corporate workforce, concentrated in cities such as Bengaluru, Gurugram, Mumbai, Hyderabad, Pune, and Chennai, operates within work cultures that prize long hours, constant availability, and uninterrupted productivity, conditions that interact uneasily with intensifying heat, water stress, and climate-induced disruption.
While corporate offices are often air-conditioned, the assumption that this constitutes meaningful protection ignores how climate stress is distributed across the entire day. Prolonged exposure to extreme heat during commutes, particularly in cities where summer temperatures routinely exceed 40 degrees Celsius, places physiological stress on bodies before and after work, a burden that is amplified for women who are pregnant, anaemic, or managing chronic health conditions. IMD data shows that several major Indian cities now experience longer and more intense heat seasons, with high night-time temperatures that reduce the body’s ability to recover from daytime exposure, even when indoor cooling is available intermittently.

Corporate women’s vulnerability is further shaped by work cultures that implicitly penalise slowing down. Pregnancy in professional settings is often managed discreetly, with women continuing long hours, frequent travel, and high cognitive load well into pregnancy, particularly in competitive sectors such as consulting, finance, technology, law, and media, where visibility and perceived commitment carry career consequences. Climate stress compounds this pressure by increasing fatigue, dehydration, and sleep disruption, yet these effects are rarely recognised as occupational health concerns, instead being individualised as stress management or work–life balance issues.
Mental health represents another under-acknowledged dimension of climate exposure for professional women. Rising temperatures, climate anxiety, and repeated exposure to climate-related disruption in cities, including floods, water shortages, and infrastructure breakdowns, contribute to chronic stress that intersects with gendered expectations of performance both at work and at home. Corporate women often shoulder a disproportionate share of unpaid care and household management even while working full time, a burden that intensifies during climate events when domestic systems falter, schools close, or household support becomes unreliable.
Corporate policies, where they exist, tend to frame climate stress as a business continuity issue rather than as a worker health issue, focusing on remote work arrangements, power backups, and office safety while leaving reproductive health, pregnancy-related accommodations, and climate-sensitive workload adjustments largely unaddressed. Maternity policies remain focused on leave duration rather than on conditions during pregnancy, and occupational health frameworks rarely incorporate environmental stressors such as extreme heat as relevant to women’s health outcomes.

What emerges is a form of climate vulnerability that is quieter and more socially acceptable, because it does not resemble deprivation, yet it follows the same underlying logic: women are expected to absorb environmental stress privately so that institutions, whether households, markets, or corporations, can continue to function without interruption. In this context, resilience is not demanded through physical endurance alone, but through sustained performance under conditions that increasingly strain the body and mind.
Conclusion
Climate change is already reshaping women’s health outcomes in India through mechanisms that remain poorly captured by existing policy frameworks. Gendered labour patterns intensify exposure, reproductive health risks are negotiated privately under climate stress, and systems appear resilient because the most consequential impacts are displaced into bodies rather than institutions.
India’s climate and health policies reflect real progress and serious intent, and these achievements should be acknowledged. Yet until women’s reproductive health is treated as a sentinel indicator of climate stress rather than as collateral impact, resilience will continue to be measured in institutional terms while its costs are borne elsewhere. Addressing this gap does not require dismantling existing frameworks, but recalibrating them to account for timing, continuity, and gendered exposure as central components of climate risk.
The challenge ahead is no longer whether India can manage climate shocks, but whether it is willing to recognise and govern the quieter, cumulative forms of harm on which its current success rests.
Sources and Further Reading
- National Family Health Survey (NFHS-5):
https://rchiips.org/nfhs/NFHS-5Reports/NFHS-5_INDIA_REPORT.pdf - India Meteorological Department, Heatwave Trends:
https://mausam.imd.gov.in - National Action Plan on Climate Change (NAPCC):
https://moef.gov.in/en/division/climate-change-division/national-action-plan-on-climate-change/ - National Action Plan on Climate Change and Human Health (NAPCCHH):
https://ncdc.gov.in/index1.php?lang=1&level=1&sublinkid=1335&lid=1143 - National Disaster Management Authority, Heat Wave Guidelines:
https://ndma.gov.in/Natural-Hazards/Heat-Wave - ORF, Climate Change and Women:
https://www.orfonline.org/expert-speak/climate-change-and-women - CSIS, Climate Crisis Jeopardizes Health in India:
https://features.csis.org/climate-crisis-jeopardizes-health-in-india/ - WHO, Climate Change and Health:
https://www.who.int/news-room/fact-sheets/detail/climate-change-and-health - World Bank, Climate Change and Poverty:
https://www.worldbank.org/en/topic/climatechange/brief/climate-change-and-poverty
